PART TWO
The Transoral Approach: From Laser to Robots
One of the first operations an ENT-head and neck surgeon learns is tonsillectomy, performed with a headlight and without magnification. Great for recurrent tonsillitis, not so good for cancer. The reason being that cancer invades the muscle under the tonsil which is not removed in a routine tonsillectomy. So, to be sure the cancer was removed we approached them through the neck, as discussed in Part 1.
The transoral excision of oropharyngeal cancers is now dominated by robotic surgery. Prior to the introduction of the da Vinci robotic platform, many ENT-head and neck surgeons were using the CO2 laser mounted on an operating microscope to successfully remove oropharyngeal cancers. This type of surgery was termed transoral laser surgery (TOLS). This approach was time-consuming and ergonomically difficult. It required a new understanding of the anatomy of the tonsil tissue and the base of tongue. Those of us who do this surgery are operating from inside out rather than outside in (the open approach).
The traditional (multiport) robotic approach to the oropharynx
The advantages of Transoral Robotic Surgery (TORS) are a crystal clear, magnified view of the oropharynx allowing the surgeon to see the extent of the cancer, the ability to use both of the surgeon’s “hands”, operating time is faster, a tracheotomy is not required, no reconstruction is required and most patients return to an oral diet within days of surgery.
The da Vinci robotic platform combined a 3D telescope with powerful computer image processing, to enable the surgeon to be immersed in a 3D operating environment. This was combined with a multi armed surgical robot, utilising 8 mm wristed instruments. These instruments functioned in the same way as the human wrist and had the added advantage of having 7 degrees of movement, compared to the 5 degrees of movement of the human wrist.
Transoral robotic surgery (TORS) relies on good exposure of the oropharynx using a variety of retractors. Three robotic arms are utilised. One arm holds the rigid 3D telescope, and the other two arms hold the instrumentation. The instruments are inserted into the mouth via three separate ports.
The surgeon sits at the operative console, controlling the surgical instruments and camera using both hand controllers and foot controls in a classic master slave relationship. Using motion scaling the quite large movements at the console are translated into small precise movements of the wristed surgical instruments. A bedside assistant sits at the head of the operating table helping to evacuate smoke and control bleeding. A scrub nurse handles the surgical and robotic instrumentation.
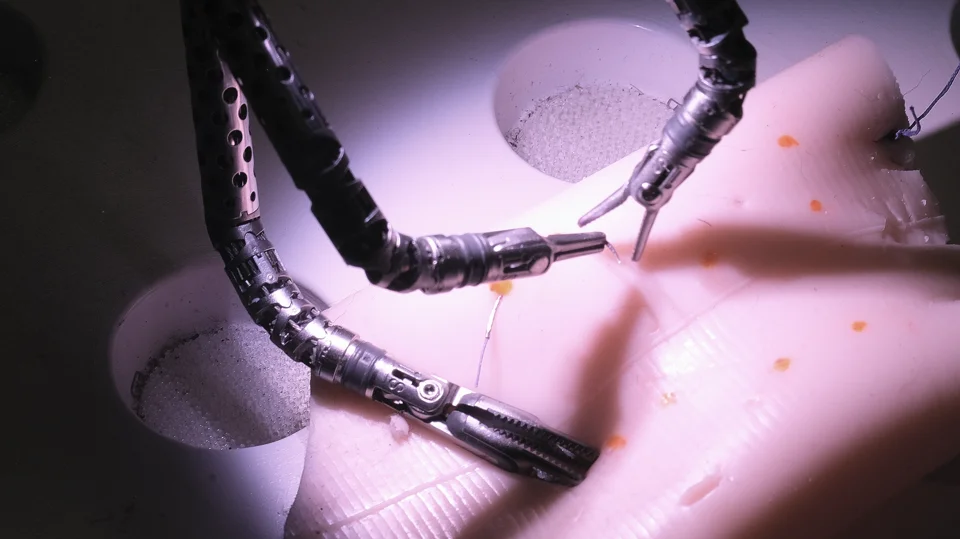
The introduction of the single port surgical robot
The creation of the da Vinci single port (SP) robot is a significant advance in the management of oropharyngeal carcinoma. Instead of three separate ports which must be angled to place instruments into the oropharynx, the SP as the name implies relies on a single port with a flexible camera and three surgical instruments.
I recently travelled to Strasburg, France to undertake training on the SP robot at the internationally recognised IRCAD: Minimally Invasive Surgery (MIS) training centre. I had already done some basic training on the SP, as well as simulation in Sydney prior to the trip. The training lab is one of the most advanced in the world. Utilising the SP in the laboratory and performing live surgery really brought home the significant advantages of the SP over the multiport robot.
The big advantage of the SP robot is the deployment of the camera and surgical arms is from a single port making the passage of instrumentation into the oropharynx and larynx easier. It also reduces the clashing of instrumentation which typically occurred with the multiport robot. The 3D camera enables an improved view of the anatomy of the oropharynx and larynx making surgery easier, more accurate and safer. The ability to use three surgical instruments instead of two helps with retracting tissues and is like having another assistant. The instruments are also smaller, at 6 mm diameter instead of 8 mm. In an area where every millimetre of room counts, this becomes important in combination with the flexible telescope.
Conclusion
The management of oropharyngeal cancer has undergone a huge change over my career. As you can see, TORS is minimally invasive surgery which continues to evolve. Providing patients with an increased number of options for management of oropharyngeal cancer. This is particularly important for those diagnosed with HPV associated oropharyngeal squamous cell carcinoma. This is a highly curable cancer and surgery alone for the right patient may be all the treatment that is required for cure. That is why it is important to seek out experienced TORS surgeons who work within a multidisciplinary team so that you are given, if appropriate, the option of surgical cure.


